


Snoring, Sinus & ENT Specialist
- Dr Kenny Peter Pang
- Ear, Nose & Throat Consultant
- Otorhinolaryngologist
- MBBS MRCS(Edinburgh)(UK)
- FRCS(Edinburgh)(UK)
- FRCS(Ireland)(OTO)
- Masters Medicine (ORL)
- Founder, ASEAN Sleep Surgical Society
- Founding Member, International Surgical Sleep Society
- Member, American Academy Sleep Medicine
- Member, Singapore Sleep Society
- Member, World Sleep Society
- Board Member, Italian Sleep Disorders Board
- Member, British Association of Sleep Surgeons
- Member, European Academy of Sleep Medicine
Thyroidectomy Surgery


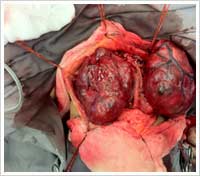


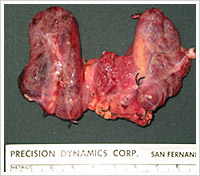
In general, most thyroid surgeons would perform a hemi-thyroidectomy first, with intra-operative frozen section (quick analysis of the thyroid specimen, nodule, lump, lobe removed) and decide to proceed with a total thyroidectomy or not, while the patient is still asleep (under anaesthesia).
Based on the frozen section, the surgeon would know if the tumour was benign (not cancer) or malignant (cancer). This would help the surgeon decide what surgery to perform.
- Neck Dissection – surgery done to removed the involved lymph nodes in the neck of the same side as the thyroid cancer. This is not often required, but occasionally, when the thyroid nodule is cancerous and has lymph node spread already, the surgeon may be required to operate on the lymph nodes of the neck, in order to remove them (for complete cancer clearance).
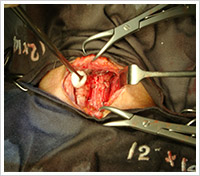

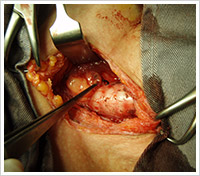
Minimally Invasive Thyroid Surgery
New technique pioneered and researched in the Medical College of Georgia, where Dr Kenny Pang was trained, together with Professor David Terris.
Endoscopic Video Assisted Thyroid Surgery:
- Smaller incision
- Less tissue trauma
- Less bleeding
- Smaller scar
- Less chance of keloid formation
- May be done as day surgery (no hospitalization)
- More cosmetic result
- Newer technique
Medical College of Georgia (MCG) has published one of the largest series of patients who underwent this new Endoscopic Minimally Invasive technique.
Thyroid Radioactive Iodine
Radioactive iodine (131I) targets the thyroid gland and has been show to play an effective role in the treatment of differentiated papillary and follicular cancers. Simultaneously, this radioisotope hones in on the salivary glands where it is concentrated and secreted into the saliva. Dose related damage to the salivary parenchyma results from the (131I) irradiation. Salivary gland swelling and pain, usually involving the parotid, can be seen. The symptoms may develop immediately after a therapeutic dose of 131I and/or months later and progress in intensity with time.
Radioactive Iodine is usually used, as an adjuvant (addition) after Total Thyroidectomy surgery and complete removal of the thyroid gland in the neck. It can also be used to treat thyroid cancer that has spread to other parts of the body.
Radioactive Iodine can be used for patients who are not willingly for surgery, or who are not fit for surgery, due to other medical problems.
Complications Of Thyroid Surgery
Complications of thyroid surgery are uncommon, but has to be discussed and made known to the patient.
- Recurrent Laryngeal Nerve Injury – this is the nerve that provides muscle movement to the voice box. Injury or involvement of this nerve would lead to hoarseness of voice (usually transient and spontaneously recovers). The overall risk is about 2%.
- Calcium Metabolism – only for total thyroid surgery. Injury to the parathyroid glands (these are small glands located very close to the thyroid gland, that are involved in calcium metabolism), might result in low calcium levels. This is usually treated with simple calcium oral medication.
- General Complications – wound infection (not common), post-surgery bleeding (related to blood oozing and slippage of sutures), neck scar formation (keloid).
- Thyrotoxic storm is an unusual complication of thyroid surgery. This condition may result from manipulation of the thyroid gland during surgery in the patients with hyperthyroidism. It can develop preoperatively, intraoperatively, or postoperatively. Prevention is the best treatment. The surgeon would prepare the patient carefully and ensure that all thyroid levels are normal before surgery.
References:
Ceresini G, Corcione L, Morganti S, et al. Ultrasound-guided fine-needle capillary biopsy of thyroid nodules, coupled with on-site cytologic review, improves results. Thyroid. May 2004;14(5):385-9.
Harvey HK. Diagnosis and management of the thyroid nodule: an overview. Otolaryngol Clin North Am. Apr 1990;23(2):303-37
Singer PA. Evaluation and management of the solitary thyroid nodule. Otolaryngol Clin North Am. Aug 1996;29(4):577-91
Sabel MS, Staren ED, Gianakakis LM, et al. Effectiveness of the thyroid scan in evaluation of the solitary thyroid nodule. Am Surg. Jul 1997;63(7):660-3; discussion 663-4
