


Snoring, Sinus & ENT Specialist
- Dr Kenny Peter Pang
- Ear, Nose & Throat Consultant
- Otorhinolaryngologist
- MBBS MRCS(Edinburgh)(UK)
- FRCS(Edinburgh)(UK)
- FRCS(Ireland)(OTO)
- Masters Medicine (ORL)
- Founder, ASEAN Sleep Surgical Society
- Founding Member, International Surgical Sleep Society
- Member, American Academy Sleep Medicine
- Member, Singapore Sleep Society
- Member, World Sleep Society
- Board Member, Italian Sleep Disorders Board
- Member, British Association of Sleep Surgeons
- Member, European Academy of Sleep Medicine
What Is A Thyroid Gland?
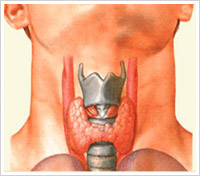
This gland is found in the neck below the mouth and just above the chest (rib cage) in the middle of the neck.
The thyroid controls how quickly the body burns energy (metabolic rate), makes proteins, and how sensitive the body should be to other hormones.
The thyroid produces thyroid hormones, principally :
- Thyroxine (T4) and
- Triiodothyronine (T3)
These hormones regulate the rate of metabolism and affect the growth and rate of function of many other systems in the body.
Iodine is an essential component of both T3 and T4. The thyroid also produces the hormone calcitonin, which plays a role in calcium homeostasis (calcium balance in the body).
The thyroid gland gets its name from the Greek word for "shield", after its shape, a double-lobed structure shaped like a letter “H”.
Hyperthyroidism (overactive thyroid) and hypothyroidism (underactive thyroid) are the most common problems of the thyroid gland.
Are There Any Thyroid Tests?
Investigation of this thyroid nodule would be the next step in the management of the patient with a neck lump. The main 2 work horses in the diagnosis of a thyroid lump would be the (1) Fine Needle Aspiration Cytology (FNAC) and the (2) Ultrasonography of the thyroid.
Fine Needle Aspiration Cytology (FNAC) has emerged as the most important step in the diagnostic evaluation of thyroid nodules. Data from numerous studies have established FNAB as highly accurate, with mean sensitivity higher than 80% and mean specificity higher than 90%. The accuracy of FNAB in diagnosing thyroid conditions highly depends on the cytopathologist's expertise and experience and the technical skill of the physician performing the biopsy. The FNAC result would be able to distinguish the following diagnostic categories: malignant (cancer), benign (non-cancer), thyroiditis (inflammation), follicular neoplasm, suspicious, or non-diagnostic. FNAC may also distinguish papillary carcinoma, medullary carcinoma, anaplastic carcinoma, and carcinoma metastatic to the thyroid gland, and it can be used to distinguish malignant lymphoma from other disease.
Possible FNAC results:
- Papillary thyroid cancer likely – needs surgery
- Follicular lesion (uncertain cancer or benign adenoma) – needs surgery
- Medullary thyroid cancer – needs surgery and blood pressure and other endocrine screening
- Small undifferentiated cancer cells seen – may need CT scan of the thyroid to see spread and may require surgery
- Inflammatory cells – may be thyroiditis, inflammation of the thyroid, may not need surgery
- Red blood cells seen only – may need to repeat test again
- Cystic Colloidal fluid – can observe for 3 months, may not need surgery
Ultrasonography (U/S) is highly sensitive in determining the size and number of thyroid nodules. Ultrasonography, on its own, cannot reliably be used to distinguish a benign nodule from a malignant nodule. The ultrasound of the thyroid would be able to show:
- The consistency of the thyroid nodule, whether it is a solid nodule, a predominantly cystic one, or a mixed nodule. Nodules that are predominantly solid have a higher chance of being cancerous, while cystic lumps are less likely to be cancerous.
- Calcifications are also another characteristic that is looked out for in a thyroid lump. Calcifications seen within the lump (intra-lesional calcium) may be suspicious, while calcium deposits around the edge of the lump (peri-lesional calcium) are less likely to be cancerous. Papillary thyroid cancer has been known to have micro-calcification within the nodule.
- Blood flow, with the Duplex ultrasound features, one is able to tell if the tumour is very vascular or not.
Computed Tomography (CT) scan of the thyroid gland is generally not cost-effective in the initial evaluation of thyroid nodules. These CT studies may be useful in the assessment of thyroid masses that are:
- suspected to be substernal,
- may have associated lymph nodes or
- my have local spread into the trachea (wind pipe) or oesophagus (gullet).
