


Snoring, Sinus & ENT Specialist
- Dr Kenny Peter Pang
- Ear, Nose & Throat Consultant
- Otorhinolaryngologist
- MBBS MRCS(Edinburgh)(UK)
- FRCS(Edinburgh)(UK)
- FRCS(Ireland)(OTO)
- Masters Medicine (ORL)
- Founder, ASEAN Sleep Surgical Society
- Founding Member, International Surgical Sleep Society
- Member, American Academy Sleep Medicine
- Member, Singapore Sleep Society
- Member, World Sleep Society
- Board Member, Italian Sleep Disorders Board
- Member, British Association of Sleep Surgeons
- Member, European Academy of Sleep Medicine
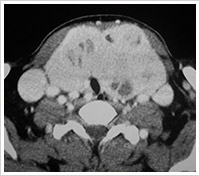
Management of the thyroid lesion (see flow chart) would depend on its cause and histology. Thyroid nodules are found in up to 7% of the population. Only 4-6.5% of these nodules are malignant. Malignant tumors of the thyroid account for only about 1% of all cancers and only 0.4% of cancer-related deaths.
There are 2 main broad categories of thyroid tumours:
- Well differentiated thyroid cancer – papillary thyroid cancer & follicular thyroid cancer
- Undifferentiated thyroid cancer – medullary thyroid cancer, anaplastic thyroid cancer, and thyroid lymphoma
Overall, in general, the good prognostic factors in thyroid cancer that one would look out for would be:
- Age (between 20 years of age to 70 years of age is better)
- Gender (female gender is better)
- Extend of tumour (no local spread is better)
- Size of nodule (less than 4cm is better)

Papillary Thyroid Carcinoma
Papillary thyroid carcinoma accounts for about 75 to 80% of all thyroid carcinomas in the world. The tumor most often occurs in individuals aged 20-50 years. In adults, the female-to-male ratio of clinically diagnosed papillary carcinoma of the thyroid is 4:1.
- The etiology of papillary thyroid is believed to be linked genetically and related to previous radiation to the head and neck region.
- Papillary thyroid cancer has a propensity to spread to the lymph nodes in the neck.
- It also has very good prognosis when diagnosed and treated early. The estimated overall 20 year survival for papillary thyroid cancer is about 90 to 95%.
- Treatment mainly consists of surgical removal of the involved thyroid lobe (hemi-thyroidectomy) and/or removal of the entire thyroid gland (total thyroidectomy).
- Some authorities have showed that the hemi-thyroidectomy would suffice for a patient with papillary thyroid cancer and good prognostic factors (namely female gender, age less than 40 years old, small tumour less than 4cm, and confined within the thyroid lobe).
- Micro-papillary thyroid cancer are papillary cancers less than 1cm in size, these have extremely good prognosis and may only require a hemi-thyroidectomy.
Follicular Thyroid Cancer
Follicular thyroid cancer is the second commonest thyroid malignancy. It would account for about 20 to 25% of all thyroid cancers encountered. In older adults, follicular thyroid cancer tends to occur more frequently than papillary carcinoma. The age range includes 30 to 60 years, mean age of about 49 years old.
- Unlike papillary thyroid cancer, follicular thyroid cancer has a propensity to spread within the blood stream to distant parts of the body; this would explain, some patients presenting with bone spread at initial diagnosis.
- In general, it also has fairly good prognosis when diagnosed and treated early.
- Treatment would consist of surgical removal of the involved thyroid lobe (hemi-thyroidectomy) and/or removal of the entire thyroid gland (total thyroidectomy).
- Some authorities have showed that a hemi-thyroidectomy would suffice for a patient with the minimally invasive follicular thyroid cancer (which could be treated as a benign tumour).
Medullary Carcinoma Of The Thyroid (MTC)
Medullary carcinoma of the thyroid (MTC) is a distinct thyroid carcinoma that originates in the parafollicular C cells of the thyroid gland. These C cells produce calcitonin. MTC has a genetic association with multiple endocrine neoplasia (MEN). Two types of MTC exists:
- Familial MTC (25% of all MTC)
- Isolated MTC (75% of all MTC)
Isolated MTC typically demonstrates a relatively indolent biologic progression. While regional lymph node metastases are possible, the lesion may not spread outside of the cervical region until several months later. MTC associated with MEN syndromes may have a more aggressive course, which also depends on associated comorbidity (eg, pheochromocytoma).
- Serum calcitonin levels may be useful to detect subclinical disease in the thyroid gland, cervical lymph nodes, or at distant sites.
- Traditionally, the pentagastrin-induced rise in calcitonin secretion has been used to diagnose medullary thyroid carcinoma (MTC).
- Treatment would consist of surgical removal of the involved thyroid lobe (hemi-thyroidectomy) and/or removal of the entire thyroid gland (total thyroidectomy); and removal of the neck lymph nodes if they are involved.
Anaplastic Carcinoma Of The Thyroid (ATC)
Anaplastic carcinoma of the thyroid (ATC) is the most aggressive thyroid gland malignancy. Although ATC accounts for less than 2% of all thyroid cancers, it causes up to 40% of deaths from thyroid cancer.
- ATC has a rapid course and early spread to other parts of the body.
- The most common sites of distant spread include (in descending order) lung, bone, and brain.
- Metastases (spread) (particularly in the lung) are likely to be present at diagnosis more than 50% of the time.
- The overall 5-year survival rate is reportedly less than 10%, and most patients do not live longer than a year after diagnosis.
- Treatment is mostly palliative •Surgery in conjunction with radiation and chemotherapy, may be required.
